百时美施贵宝nivolumab+Yervoy组合疗法Ib期1年总生存率高达94%
来源:生物谷 2014-06-04 08:59
2014年6月4日讯 /生物谷BIOON/ --百时美施贵宝(BMS)6月2日公布了一项多组Ib期剂量范围试验Study-004的随访数据。该研究在晚期黑色素瘤患者中开展,调查了实验性PD-1免疫检查点抑制剂nivolumab和黑色素瘤药物Yervoy(ipilimumab)同时给药或先后给药的安全性和疗效。对nivolumab(1mg/kg)+Yervoy(3mg/kg)同时给药组的随访数据表明,该治疗组患者一年总生存率(OS)达94%,两年总生存率达88%。这一剂量方案已用于正在开展的II期和III期临床试验。同时给药组中,未出现新的安全性信号。相关数据已提交至美国临床肿瘤学会(ASCO)第50届年会上。
关于Nivolumab(BMS-936559):
癌细胞可能利用“调节子(regulator)”途径,如检查点(checkpoint)途径,逃避机体免疫系统,保护肿瘤免受免疫攻击。
Nivolumab是一种实验性、全人源化IgG4、抗程序性死亡受体1(PD-1)单克隆抗体,能够抑制PD-1与程序性死亡配体1(PD-L1/B7-H1)和程序性死亡配体2(PD-L2/B7-DC)的结合。阻断PD-1与其配体的相互作用,可能使T细胞恢复抗肿瘤免疫应答。目前,百时美施贵宝正调查nivolumab用于恶性黑色素瘤、肾癌、非小细胞肺癌及其他癌症的治疗。
nivolumab的开发项目研究总数超过25个:调查作为单药疗法或与其他药物联合用药,用于多个肿瘤类型的治疗,包括:非小细胞肺癌、小细胞肺癌、黑色素瘤、肾细胞癌、肝癌、血液癌症、三阴性乳腺癌、胃癌、胰腺癌。
关于Yervoy:
Yervoy是一种重组人单克隆抗体,阻断细胞毒性T淋巴细胞相关抗原4(CTLA-4)。CTLA-4是一种T细胞活化的负调控因子,Yervoy与CTLA-4结合后,能阻断CTLA-4与其配体CD80/CD86的相互作用。阻断CTLA-4已被证明能够增强T细胞的活化和增殖。Yervoy在黑色素瘤患者中的疗效作用机制,是间接通过T细胞介导的抗肿瘤免疫反应。FDA于2011年3月批准Yervoy 3mg/kg单药疗法用于不能手术切除或转移性黑色素瘤患者的治疗,目前该药已获全球40多个国家批准。(生物谷Bioon.com)
英文原文:One- & Two-Year Survival Rates of 94% and 88% Announced from Phase 1b Trial of Investigational PD-1 Checkpoint Inhibitor Nivolumab and Yervoy® (ipilimumab) in Advanced Melanoma; Ongoing Phase 2/3 Trials to Confirm Results
PRINCETON, N.J.--(BUSINESS WIRE)--Bristol-Myers Squibb Company (NYSE: BMY) today announced follow up results from Study -004, a multi-arm Phase 1b dose-ranging trial evaluating the safety and activity of the combination regimen of nivolumab, an investigational PD-1 immune checkpoint inhibitor, and Yervoy® (ipilimumab) given either concurrently or sequentially in patients with advanced melanoma (n=127). After an additional year of follow up of the cohort that received the concurrent combination regimen of nivolumab 1 mg/kg plus Yervoy 3mg/kg (n=17), the one-year overall survival (OS) rate was 94% and the two-year OS rate was 88%. These are the doses used in the ongoing Phase 2 and Phase 3 trials, CheckMate -069 and -067. No new safety signals were reported in the concurrent combination cohorts with additional follow up (n=53) and grade 3-4 treatment-related adverse events (AEs) occurred in 62% of patients. The most common were asymptomatic increases in lipase (15%), ALT (12%) and AST (11%). These data will be presented today at the 50th Annual Meeting of the American Society of Clinical Oncology (ASCO) and featured during an ASCO press briefing at 8 a.m. CDT (Abstract # LBA9003).
“The treatment of advanced melanoma has changed dramatically in the last few years, but there continues to be a need to increase the number of patients who experience a long-term survival benefit,” said Dr. Mario Sznol, Yale University School of Medicine and Yale Cancer Center, presenter of the results. “While these are Phase 1b data, the duration of response and one- and two-year survival rates observed with the combination regimen of nivolumab and Yervoy are very encouraging and support the rationale for the ongoing, late stage trials of this combination regimen.”
“The science of immuno-oncology – harnessing the patient’s immune system to treat cancer – is rapidly evolving,” said Michael Giordano, senior vice president, Head of Development, Oncology & Immunology at Bristol-Myers Squibb. “These results are the most advanced data set to date evaluating the potential of combining immune checkpoint inhibitors. As leaders in the field, they reinforce our aspiration that combining immunotherapies may be foundational and may have the potential to change the standard of care by transforming survival expectations.”
Results from Phase 1b Combination Regimen (Study -004)
Study 004 is a dose-ranging Phase 1 study (n=127) evaluating the safety, antitumor activity and pharmacokinetics of the combination regimen of nivolumab and Yervoy given concurrently or sequentially in patients with advanced melanoma. Prior to enrollment, patients could have received up to three systemic therapies.
In the concurrent regimen cohort (n=53), eligible patients received nivolumab and Yervoy every three weeks for four doses, followed by nivolumab alone every three weeks for four doses. This concurrent combination regimen treatment was subsequently continued every 12 weeks for up to eight doses. Cohorts of a maximum of 17 patients per dose level were enrolled (nivolumab 0.3 mg/kg + Yervoy 3 mg/kg [n=14]; nivolumab 1 mg/kg + Yervoy 3 mg/kg [n=17]; nivolumab 3 mg/kg + Yervoy at an investigational dose of 1 mg/kg [n=16]; nivolumab 3 mg/kg + Yervoy 3 mg/kg [n=6]). In an expansion cohort (n=41), eligible patients received the concurrent combination regimen of nivolumab 1 mg/kg and Yervoy 3 mg/kg every three weeks for four doses, followed by nivolumab alone at 3 mg/kg every two weeks until progression, which is the same schedule utilized in the ongoing Phase 2 and Phase 3 trials. In the sequenced regimen cohort (n=33), patients previously treated with Yervoy received nivolumab alone at 1 mg/kg or 3 mg/kg every two weeks.
Results from this trial were first published in the New England Journal of Medicine and presented at ASCO in 2013. The updated data, including those shown below, are based on a median follow up of 22 months and reflect an additional year of follow up from patients initially enrolled in the trial.
Efficacy Summary: Concurrent and Sequenced Cohorts
Nivolumab (mg/kg) + Yervoy (mg/kg) [n] ORR, % CR, % 1-Year OS, % 2-Year OS, %
Concurrent Cohorts [53] 42 17 85 79
0.3 + 3 [14] 21 14 57 50
1 + 3 [17] 53 18 94 88
3 + 1 [16] 44 25 94 NC
3 + 3 [6] 50 0 100 NC
Expansion 1 + 3 [41] 43 10** NC NC
Sequenced Cohort [33] 31 3 70 [23] NC
NC: Not calculated/insufficient follow up; ORR: objective response rate; CR: complete response
**Two unconfirmed responses
Responses were observed regardless of BRAF mutational status or PD-L1 expression.
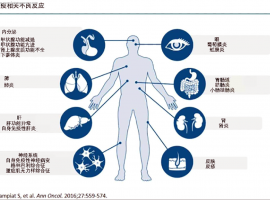
No new safety signals were reported with additional follow up. Grade 3-4 treatment-related AEs occurred in 62% of patients in the concurrent cohorts, managed with standard algorithms. The most common were asymptomatic increases in lipase (15%), ALT (12%) and AST (11%). Twenty-two patients (23%) discontinued treatment due to related AEs. There was one drug-related death due to fatal multi-organ failure following an initial event of colitis.
About Advanced Melanoma
Melanoma is a form of skin cancer characterized by the uncontrolled growth of pigment-producing cells (melanocytes) located in the skin. Metastatic melanoma is the deadliest form of the disease, and occurs when cancer spreads beyond the surface of the skin to other organs, such as the lymph nodes, lungs, brain or other areas of the body. The incidence of melanoma has been increasing for at least 30 years. In 2012, an estimated 232,130 melanoma cases were diagnosed globally. Melanoma is mostly curable when treated in its early stages. However, in its late stages, the average survival rate has historically been just six months with a one-year mortality rate of 75%, making it one of the most aggressive forms of cancer.
About Bristol-Myers Squibb Immuno-Oncology Trials in Melanoma
Bristol-Myers Squibb is committed to the research and development of immuno-oncology as an innovative approach to treating melanoma and has a broad development program evaluating its approved and investigational immunotherapies – either as single agents or as part of a regimen - across lines of therapy, stages of disease and biomarker expression. Among these are five Phase 3 trials. There are two ongoing Phase 3 trials evaluating nivolumab as a single agent at the 3 mg/kg dose in treatment-naïve patients (CheckMate -066) as well as in patients who have been previously treated (CheckMate -037). A Phase 3 trial evaluating Yervoy 3 mg/kg vs. Yervoy 10 mg/mg in patients with previously treated or treatment-naïve metastatic melanoma is ongoing (Study -169) and the first results of a Phase 3 trial evaluating the investigational use of Yervoy 10 mg/kg in patients with Stage 3 melanoma who are at high risk of recurrence following complete surgical resection (Study -029) will be featured today during an ASCO press briefing at 8 a.m. CDT and presented in an oral session at 3 p.m. CDT (Abstract #LBA9008). Additionally, a Phase 3 trial evaluating the combination regimen of nivolumab and Yervoy in treatment-naïve patients is ongoing (CheckMate -067).
About Nivolumab and Yervoy
Cancer cells may exploit “regulatory” pathways, such as checkpoint pathways, to hide from the immune system and shield the tumor from immune attack. Nivolumab and Yervoy are both monoclonal antibodies and immune checkpoint inhibitors, but target different receptors for distinct T-cell checkpoint pathways.
Nivolumab is an investigational, fully-human PD-1 immune checkpoint inhibitor that binds to the checkpoint receptor PD-1 (programmed death-1) expressed on activated T-cells. We are investigating whether by blocking this pathway, nivolumab would enable the immune system to resume its ability to recognize, attack and destroy cancer cells.
Bristol-Myers Squibb has a broad, global development program to study nivolumab in multiple tumor types consisting of more than 35 trials – as monotherapy or in combination with other therapies – in which more than 7,000 patients have been enrolled worldwide. Among these are several potentially registrational trials in non-small cell lung cancer (NSCLC), melanoma, renal cell carcinoma (RCC), head and neck cancer, glioblastoma and non-Hodgkin lymphoma. In 2013, the FDA granted Fast Track designation for nivolumab in NSCLC, melanoma and RCC. Earlier this month, the FDA granted nivolumab Breakthrough Therapy Designation for the treatment of patients with Hodgkin lymphoma after failure of autologous stem cell transplant and brentuximab.
Yervoy, which is a recombinant, human monoclonal antibody, blocks the cytotoxic T- lymphocyte antigen-4 (CTLA-4). CTLA-4 is a negative regulator of T-cell activation. Ipilimumab binds to CTLA-4 and blocks the interaction of CTLA-4 with its ligands, CD80/CD86. Blockade of CTLA-4 has been shown to augment T-cell activation and proliferation. The mechanism of action of ipilimumab’s effect in patients with melanoma is indirect through T-cell mediated anti-tumor immune responses. On March 25, 2011, the FDA approved Yervoy 3 mg/kg monotherapy for patients with unresectable or metastatic melanoma. Yervoy is now approved in more than 40 countries.
YERVOY® (ipilimumab) INDICATION & IMPORTANT SAFETY INFORMATION
YERVOY (ipilimumab) is indicated for the treatment of unresectable or metastatic melanoma. |
 跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
 egfr19突变,16个月耐药,后续该如何
2023.7月爸爸确诊肺癌晚期,全身多处骨转 脑转,基因检测egfr19突变,单用阿美11个月
egfr19突变,16个月耐药,后续该如何
2023.7月爸爸确诊肺癌晚期,全身多处骨转 脑转,基因检测egfr19突变,单用阿美11个月
![[9.20更新紧急求助]K药单免,肺部大幅缩小但脑部进展](data/attachment/block/78/78b79df7f93e2c961326f54ecb07af7c.jpg) [9.20更新紧急求助]K药单免,肺部大
我父亲5月30,6月20,分别使用两次K药治疗。后因为肠道免疫副反应停止了K药直到现在.
[9.20更新紧急求助]K药单免,肺部大
我父亲5月30,6月20,分别使用两次K药治疗。后因为肠道免疫副反应停止了K药直到现在.
 免疫治疗的副作用有何征兆?可以预防
我们常说的抗肿瘤免疫治疗,多指以PD-1/PD-L1抑制剂为代表的免疫抑制剂,通过激活患
免疫治疗的副作用有何征兆?可以预防
我们常说的抗肿瘤免疫治疗,多指以PD-1/PD-L1抑制剂为代表的免疫抑制剂,通过激活患
 建议收藏!肺癌ALK患者靶向药耐药后
作者:闵
ALK突变常被众多病友称为“钻石突变”,不单是由于对应的靶向药价格高昂,更
建议收藏!肺癌ALK患者靶向药耐药后
作者:闵
ALK突变常被众多病友称为“钻石突变”,不单是由于对应的靶向药价格高昂,更








 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡


![[9.20更新紧急求助]K药单免,肺部大幅缩小但脑部进展](data/attachment/block/be/bef922fb542a7d3992f68e4d95a9703b.jpg)